About Adenomyosis
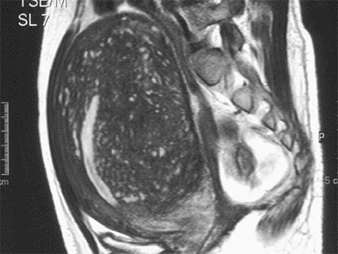
Adenomyomatous uterus
Adenomyosis is a condition where endometrial tissue, i.e., uterine lining cells, are dispersed within the muscle of the uterus. It is essentially "endometriosis" of the uterus. There is no capsule or line of demarcation between adenomyosis and the rest of the uterine muscle, like exists with the more common condition of uterine fibroids, benign muscle tumors of the uterus. Adenomyosis is an intensely painful condition, with incapacitating pain during menstruation, and prolonged menstrual bleeding. This is because normally when menstruation occurs, the uterine lining sheds and blood drains out of the uterus. But with adenomyosis, the uterine lining, or endometrial cells, that are trapped within uterine musculature, bleed but cannot drain out. So the uterus gets bigger and bigger and more and more boggy and enlarged and painful.
About the Osada Procedure
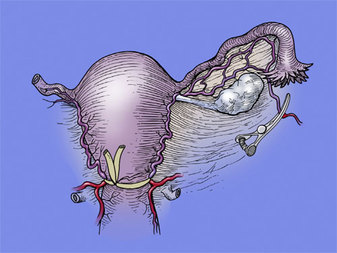
Uterine tubing tourniquet image
Usually the only solution to the misery and pain that adenomyosis can cause is considered to be hysterectomy, that is, removal of the uterus.
However many women with adenomyosis do not want to lose their uterus, and wish to be able to have children. For women who wish to become pregnant and have children, this is an awful decision to make. Yet unlike uterine myomas, or fibroids, which can easily be "shelled out" of the uterus because there is a clear line of demarcation between tumor and true uterine musculature, with adenomyosis, there is no such line of demarcation. The uterine muscle is completely infiltrated with endometriosis tissue, diffusely and throughout, and there is not even a clear demarcation of uterine lining.
However, Hisao Osada M.D., PHD. has pioneered a procedure to solve this problem. The idea is to first prevent the massive bleeding this operation would cause by putting a temporary tourniquet around the uterus, and then to open the uterus boldly all the way down to the endometrial lining. Then the non-demarcated adenomyotic tissue is excised leaving a centimeter on the endometrial side and a centimeter on the serosal (outer) side of the uterus. Then the remaining muscle of this debulked adenomyotic uterus musculature is closed with many layers of sutures, all non-overlappying flaps, to prevent the risk of rupture.
The results are immediate and dramatic. There is almost instant relief of pelvic pain, and miserable menstrual periods, and normal periods resume with minimal pain. Furthermore, the patient is now able to get pregnant normally. She will need a C-section, but that is a small price to pay for preserving her uterus, allowing full term pregnancy, and alleviating her painful and miserable symptoms.
Currently, this approach is being performed by Prof. Osada in Japan and long time collaborator, Dr. Sherman J. Silber, M.D. at The Infertility Center of St. Louis, USA.
However many women with adenomyosis do not want to lose their uterus, and wish to be able to have children. For women who wish to become pregnant and have children, this is an awful decision to make. Yet unlike uterine myomas, or fibroids, which can easily be "shelled out" of the uterus because there is a clear line of demarcation between tumor and true uterine musculature, with adenomyosis, there is no such line of demarcation. The uterine muscle is completely infiltrated with endometriosis tissue, diffusely and throughout, and there is not even a clear demarcation of uterine lining.
However, Hisao Osada M.D., PHD. has pioneered a procedure to solve this problem. The idea is to first prevent the massive bleeding this operation would cause by putting a temporary tourniquet around the uterus, and then to open the uterus boldly all the way down to the endometrial lining. Then the non-demarcated adenomyotic tissue is excised leaving a centimeter on the endometrial side and a centimeter on the serosal (outer) side of the uterus. Then the remaining muscle of this debulked adenomyotic uterus musculature is closed with many layers of sutures, all non-overlappying flaps, to prevent the risk of rupture.
The results are immediate and dramatic. There is almost instant relief of pelvic pain, and miserable menstrual periods, and normal periods resume with minimal pain. Furthermore, the patient is now able to get pregnant normally. She will need a C-section, but that is a small price to pay for preserving her uterus, allowing full term pregnancy, and alleviating her painful and miserable symptoms.
Currently, this approach is being performed by Prof. Osada in Japan and long time collaborator, Dr. Sherman J. Silber, M.D. at The Infertility Center of St. Louis, USA.